
Journal of Vita Columbia Volume 2 Issue 1 – Clinical Nutrition
Vitamin C: An Overview – Metabolism, Toxicity, Deficiency, Involvement
January 17th, 2022
Authors:
Blessy K Joy, MBBS
Kevin Joy, BSc, DCh
Wafaa Chorfi, MD
How to cite this article:
Joy BK, Joy K, Chorfi W. Vitamin C: Metabolism, Toxicity, Deficiency, Involvement. 2022. Journal of Vita Columbia. 2(1).
Abstract:
This is a brief overview on the on water soluble molecule known as ascorbic acid, more commonly referred to as vitamin C. The following article will overview the sources of vitamin C, the appropriate dosing, metabolism, and the consequences of vitamin C toxicity and deficiency, while examining the impact it has normal physiology and its role as a therapeutic in treating certain ailments.
Introduction:
Vitamin C is a water-soluble molecule that is required to help support normal physiological functions within the body [1]. This vitamin acts as a reducing agent and provides some antioxidant properties which may help in preventing tissue damage. Also known as ascorbic acid, vitamin C can be sourced readily from common dietary sources or in the form of supplements [2]. Appropriate dosing and adequate daily intake are required to help normal bodily functions such as collagen synthesis [1,2]. While there is no gold standard to measure levels of vitamin C in the body, examining plasma levels are sufficient to determine whether hypo or hypervitaminosis C exists [7,8]. Vitamin C also plays supportive roles in physiology and as an adjunct therapeutic in numerous pathologies. All of this will be explored further in this brief overview.
Dietary Intake of Vitamin C
As Vitamin C cannot be synthesized endogenously, exogenous sources of Vitamin C are required to maintain normal levels within the body [1]. Natural food sources are the primary exogenous source for humans to obtain vitamin C. Foods such as citrus fruits, tomatoes and tomato juices, and potatoes are major sources of Vitamin C, especially in North America [3]. For reference, consuming a medium size orange provides roughly 70mg of vitamin C [4]. Some other sources of vitamin C includes fruits such as strawberries, kiwis, and cantaloupe, in addition to vegetables like green and red peppers, broccoli, spinach, cabbage, and Brussel sprouts [3,4]. Where absent, such as in grains, vitamin C can be added to foods, like cereals, in order to fortify them. Breast milk has also been found to contain vitamin C. When storing or preparing foods with vitamin C, the amount present within foods can be diminished with prolonged storage or high temperatures. Heat can destroy vitamin C, as such moderate temperature cooking such as with a microwave or through steaming can help prevent cooking losses. Dietary supplementation is another source of obtaining vitamin C and offer vitamin C in the form of ascorbic acid.
The recommended daily intake of vitamin C for adult men is 95mg/day and 75mg/day for adult women. As compiled by the National Institute of Health Office of Dietary Supplements, Table 1 references daily recommended intakes for various age demographics:
Table 1: Recommended Dietary Allowances (RDAs) for Vitamin C [3]
| Age | Male | Female | Pregnancy | Lactation |
| 0–6 months | 40 mg | 40 mg | ||
| 7–12 months | 50 mg | 50 mg | ||
| 1–3 years | 15 mg | 15 mg | ||
| 4–8 years | 25 mg | 25 mg | ||
| 9–13 years | 45 mg | 45 mg | ||
| 14–18 years | 75 mg | 65 mg | 80 mg | 115 mg |
| 19+ years | 90 mg | 75 mg | 85 mg | 120 mg |
| Smokers | Individuals who smoke require 35 mg/day more vitamin C than non-smokers. | |||
Metabolism of Vitamin C:
Vitamin C exists as two forms within the body; ascorbic acid (reduced form) and dehydroascorbic acid (oxidized form). Ascorbic acid is the predominant form that exists as most of the oxidized form is converted to ascorbic acid. Absorption of vitamin C occurs in the distal small intestine through the apical membrane of the epithelial cells through an active transport sodium symport system [5]. The body is capable of absorbing 100mg/day of vitamin C. As absorption is an enteral process, there are limits on how much can be absorbed. Anything in excess of 1g/day reduces vitamin C absorption to fifty percent, reducing the bioavailability [6].
Measurement of Vitamin C:
While no definitive methods of measurement have been established for vitamin C, several methods exist to demonstrate vitamin C markers. Plasma and leukocyte vitamin C concentrations remain the most reliable markers [7]. In measuring plasma, one can measure ascorbic acid only, assess ascorbic acid and dehydroascorbic acid separately, or evaluate the total level of vitamin C, which entails taking the sum of ascorbic acid and dehydroascorbic acid, through high-performance liquid chromatography [8]. The reference range for plasma levels of vitamin C falls between 0.4-2mg/dL [30]
Vitamin C Toxicity:
Being a water-soluble molecule, vitamin C is associated with low toxicity in comparison to the fat-soluble vitamins [1]. Most common complaints associated with excessive vitamin C intake include: diarrhea, nausea, abdominal cramping, and various gastrointestinal issues due to unabsorbed vitamin C [3,10]. There is conflicting evidence linking excessive intake with precipitation of oxalate stones in men. However, in the absence of any renal impairment, or pre-existing hyperoxaluria, this is not a concern [9]. In patients with hereditary hemochromatosis, taking vitamin C supplements is not recommended as this can cause iron overload with resultant tissue damage [3,10]. Similarly, although very rare, excessive quantities of vitamin C have been associated with fatal cardiac arrythmias in patients with iron overload. To prevent this, it is advisable to discourage pharmacological vitamin C supplementation [11].
Table 2, borrowed from the National Institute of Health Office of Dietary Supplements, provides the tolerable upper limits of vitamin C intakes of various age populations:
Table 2: Tolerable Upper Intake Levels (ULs) for Vitamin C [3]
| Age | Male | Female | Pregnancy | Lactation |
| 0–12 months | Not possible to establish* | Not possible to establish* | ||
| 1–3 years | 400 mg | 400 mg | ||
| 4–8 years | 650 mg | 650 mg | ||
| 9–13 years | 1,200 mg | 1,200 mg | ||
| 14–18 years | 1,800 mg | 1,800 mg | 1,800 mg | 1,800 mg |
| 19+ years | 2,000 mg | 2,000 mg | 2,000 mg | 2,000 mg |
Vitamin C Deficiency:
The primary outcome of vitamin C deficiency is scurvy. Scurvy can develop within one month of the body receiving little to no vitamin C [3,12,13]. Symptoms begin as fatigue and malaise with inflammation of the gums. This inflammation can progress to bleeding gums. As the deficiency progresses, collagen synthesis is weakened which contributes to poor wound healing. It is common to see petechiae, ecchymoses, and purpura, along with perifollicular hemorrhaging, bruising and even arthralgias with scurvy [13]. Bone disease can manifest in children with scurvy. Left untreated, scurvy can be fatal [12]. Consuming food sources rich in vitamin C along with supplementation can help correct scurvy when intervened in time. For pediatric cases, 100mg of ascorbic acid provided three times daily through oral, intramuscular, or intravenous methods for 1 week, and then continuous daily vitamin C intake for 1 month should help fight scurvy [14]. Adult populations need between 300-1000mg daily for 1 month to help combat scurvy [12, 13].
Certain groups are at risk for developing vitamin C deficiency. These groups include smokers and those who receive secondhand smoke on a regular basis [3]. This is due to the increased oxidative stress caused by cigarette smoke leading to diminished plasma and leukocyte vitamin C concentrations. Infants that are fed evaporated or boiled milk are at risk due to insufficient vitamin C in milk and the heating process can destroy vitamin C levels [3, 15]. People who live in areas with limited food variety can experience vitamin C deficiency and also those with malabsorptive disorders as not enough vitamin C is being absorbed by the body [3,10,12, 16].
Physiological Involvement of Vitamin C:
Vitamin C supports numerous physiological processes. Vitamin C is primarily a reducing agent, meaning it donates electrons. This function helps support and regulate copper and iron activity in the body including helping aid iron absorption [17]. Tt has antioxidant properties enabling it to reduce molecular oxygen. This antioxidant property help stabilize vitamin E and enables vitamin C to be a co-factor in reducing folate to dihydrofolate or tetrahydrofolate. Further, as a cofactor, vitamin C also helps with neurotransmitter synthesis of catecholamines, especially norepinephrine [18].
In aiding synthesis of physiological processes, vitamin C also supports fatty acid transport in helping to synthesize carnitine [19]. It is presumed that vitamin C may also play a role in prostaglandin metabolism, helping to reduce inflammation.
In discussing scurvy, one of the largest roles vitamin C plays in physiology is in help to support collagen synthesis. Where scurvy leads to collagen breakdown, adequate levels of vitamin C lead to collagen synthesis by supporting the enzymes prolyl hydroxylase and lysyl hydroxylase in forming hydroxyproline and hydroxylysine. These products are formed from the hydroxylation of proline and lysine residues respectively. The formation of these products results in collagen synthesis to maintain proper wound healing, tooth formation, and adequate bone homeostasis [20].
Therapeutic Involvement of Vitamin C:
In having an antioxidant role and having an effect on the immune system, vitamin C has been implicated in numerous pathologies. There is conflicting evidence linking vitamin C consumption with reduced cancer risk. This perceived risk reduction may be in part due to higher consumption of fruits and vegetables (source of vitamin C) however, no substantial evidence and no significant relationship exists linking cancer prevention to dietary or supplementary vitamin C [21-23].
Similarly conflicting evidence exists in examining vitamin C and cardiovascular health. There is limited evidence to show that vitamin C plays a role in reducing atherosclerosis by reducing monocyte adherence to the vascular endothelium [24]. However, many studies show that dietary vitamin C rather than supplemental vitamin C is inversely related to cardiovascular disease [25].
It is a long-held belief that increased vitamin C intake will help to treat and/or prevent the common cold. Again, the evidence is limited. A Cochrane review from 2007 [26] revealed that prophylactic use of vitamin C in the general population did not reduce the incidence of the common cold. However, in extreme physical exercise, such as marathon running or skiing, prophylactic vitamin C did exert a protective role in reducing incidence of the common cold. It is important to note that if taken after onset of the cold, vitamin C does not appear to be beneficial.
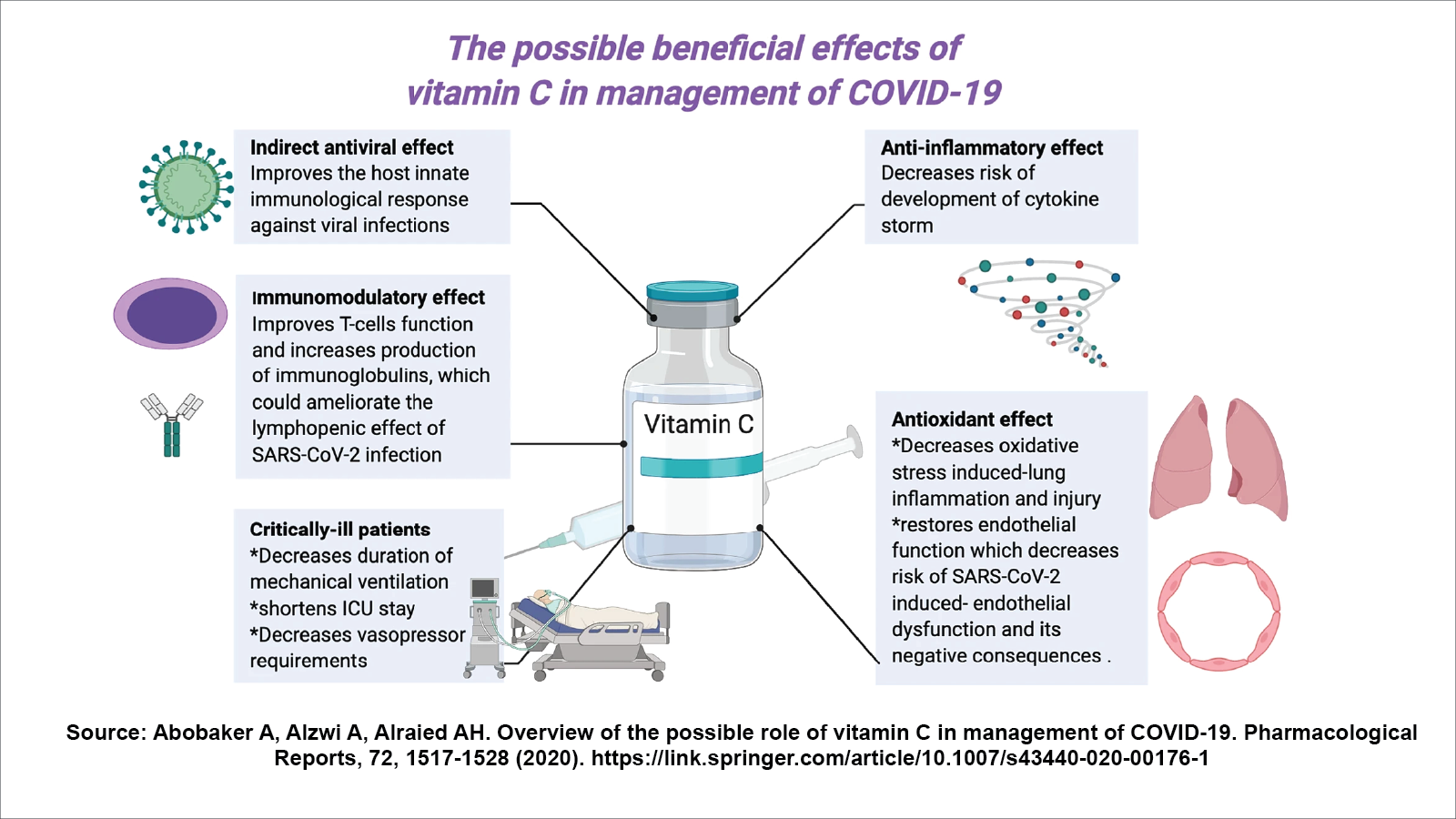
With the ongoing pandemic, it is important to examine the role vitamin C plays in treating and managing Covid-19 patients. Research is still ongoing to examine the therapeutic role of vitamin C administration for severe Covid cases, however preliminary limited research findings suggests that administration of vitamin C can lead to significantly reduced mortality. In one meta-analysis vitamin C was shown to decrease ICU stay by 8 percent [29]. It is important to note that vitamin C must be given as an adjunct to other treatment and management options [27]. Vitamin C only plays a supportive role in treating Covid. Figure 1[28] highlights some beneficial effects of vitamin C on Covid-19.
Figure 1: The possible beneficial effects of Vitamin C in the management of Covid-19 [27]
Conclusion:
Vitamin C also known as ascorbic is a water-soluble vitamin that plays a supportive role in maintaining homeostasis. Given its pleiotropic nature, the application of vitamin C within the medical setting is widespread and effective when provided as an adjunct to other treatments. It’s use as a mainstay therapeutic warrants further research consideration especially when dealing with novel pathologies such as Covid-19. Toxicity to vitamin C is rare and it can be sourced readily through regular dietary sources and supplementation. It is imperative to maintain adequate levels of vitamin C to preserve normal bodily functions.
References:
- Carr, A. C., & Maggini, S. (2017). Vitamin C and Immune Function. Nutrients, 9(11), 1211. https://doi.org/10.3390/nu9111211
- Li, Y., & Schellhorn, H. E. (2007). New developments and novel therapeutic perspectives for vitamin C. The Journal of nutrition, 137(10), 2171–2184. https://doi.org/10.1093/jn/137.10.2171
- Office of Dietary Supplements – Vitamin C. (2021). Retrieved 30 August 2021, from https://ods.od.nih.gov/factsheets/VitaminC-HealthProfessional/U.S. Department of Agriculture, Agricultural Research Service. FoodData Central, 2019.
- Lykkesfeldt, J., & Tveden-Nyborg, P. (2019). The Pharmacokinetics of Vitamin C. Nutrients, 11(10), 2412. https://doi.org/10.3390/nu11102412
- Glatthaar, B. E., Hornig, D. H., & Moser, U. (1986). The role of ascorbic acid in carcinogenesis. Advances in experimental medicine and biology, 206, 357–377. https://doi.org/10.1007/978-1-4613-1835-4_27
- Collie, J., Greaves, R., Jones, O., Eastwood, G. & Bellomo, R. (2020). Vitamin C measurement in critical illness: challenges, methodologies and quality improvements: . Clinical Chemistry and Laboratory Medicine (CCLM), 58(4), 460-470. https://doi.org/10.1515/cclm-2019-0912
- Jacob R. A. (1990). Assessment of human vitamin C status. The Journal of nutrition, 120 Suppl 11, 1480–1485. https://doi.org/10.1093/jn/120.suppl_11.1480
- Ferraro, P. M., Curhan, G. C., Gambaro, G., & Taylor, E. N. (2016). Total, Dietary, and Supplemental Vitamin C Intake and Risk of Incident Kidney Stones. American journal of kidney diseases : the official journal of the National Kidney Foundation, 67(3), 400–407. https://doi.org/10.1053/j.ajkd.2015.09.005
- Jacob, R. A., & Sotoudeh, G. (2002). Vitamin C function and status in chronic disease. Nutrition in clinical care : an official publication of Tufts University, 5(2), 66–74. https://doi.org/10.1046/j.1523-5408.2002.00005.x
- McLaran, C. J., Bett, J. H., Nye, J. A., & Halliday, J. W. (1982). Congestive cardiomyopathy and haemochromatosis–rapid progression possibly accelerated by excessive ingestion of ascorbic acid. Australian and New Zealand journal of medicine, 12(2), 187–188. https://doi.org/10.1111/j.1445-5994.1982.tb02457.x
- Weinstein, M., Babyn, P., & Zlotkin, S. (2001). An orange a day keeps the doctor away: scurvy in the year 2000. Pediatrics, 108(3), E55. https://doi.org/10.1542/peds.108.3.e55
- Hirschmann, J. V., & Raugi, G. J. (1999). Adult scurvy. Journal of the American Academy of Dermatology, 41(6), 895–910. https://doi.org/10.1016/s0190-9622(99)70244-6
- American Academy of Pediatrics Committee on Nutrition. Water-soluble vitamins. In: Pediatric Nutrition, 8th ed, Kleinman RE, Greer FR (Eds), American Academy of Pediatrics, 2019. p.655.
- Bates C. J. (1997). Bioavailability of vitamin C. European journal of clinical nutrition, 51 Suppl 1, S28–S33.
- Hoffman F. A. (1985). Micronutrient requirements of cancer patients. Cancer, 55(1 Suppl), 295–300. https://doi.org/10.1002/1097-0142(19850101)55:1+<295::aid-cncr2820551315>3.0.co;2-x
- Ross, A. C., Caballero, B., Cousins, R. J., Tucker, K. L., & Ziegler, T. R. (2012). Modern nutrition in health and disease (No. Ed. 11). Lippincott Williams & Wilkins.
- Carr, A. C., Shaw, G. M., Fowler, A. A., & Natarajan, R. (2015). Ascorbate-dependent vasopressor synthesis: a rationale for vitamin C administration in severe sepsis and septic shock?. Critical care (London, England), 19, 418. https://doi.org/10.1186/s13054-015-1131-2
- Rebouche C. J. (1995). Renal handling of carnitine in experimental vitamin C deficiency. Metabolism: clinical and experimental, 44(12), 1639–1643. https://doi.org/10.1016/0026-0495(95)90087-x
- Pinnell S. R. (1982). Regulation of collagen synthesis. The Journal of investigative dermatology, 79 Suppl 1, 73s–76s. https://doi.org/10.1111/1523-1747.ep12545835
- Long, Y., Fei, H., Xu, S., Wen, J., Ye, L., & Su, Z. (2020). Association about dietary vitamin C intake on the risk of ovarian cancer: a meta-analysis. Bioscience reports, 40(8), BSR20192385. https://doi.org/10.1042/BSR20192385
- Zhang, D., Xu, P., Li, Y., Wei, B., Yang, S., Zheng, Y., Lyu, L., Deng, Y., Zhai, Z., Li, N., Wang, N., Lyu, J., & Dai, Z. (2020). Association of vitamin C intake with breast cancer risk and mortality: a meta-analysis of observational studies. Aging, 12(18), 18415–18435. Advance online publication. https://doi.org/10.18632/aging.103769
- Parent, M. E., Richard, H., Rousseau, M. C., & Trudeau, K. (2018). Vitamin C Intake and Risk of Prostate Cancer: The Montreal PROtEuS Study. Frontiers in physiology, 9, 1218. https://doi.org/10.3389/fphys.2018.01218
- Honarbakhsh, S., & Schachter, M. (2009). Vitamins and cardiovascular disease. The British journal of nutrition, 101(8), 1113–1131. https://doi.org/10.1017/S000711450809123X
- Ye, Z., & Song, H. (2008). Antioxidant vitamins intake and the risk of coronary heart disease: meta-analysis of cohort studies. European journal of cardiovascular prevention and rehabilitation : official journal of the European Society of Cardiology, Working Groups on Epidemiology & Prevention and Cardiac Rehabilitation and Exercise Physiology, 15(1), 26–34. https://doi.org/10.1097/HJR.0b013e3282f11f95
- Douglas, R. M., Hemilä, H., Chalker, E., & Treacy, B. (2007). Vitamin C for preventing and treating the common cold. The Cochrane database of systematic reviews, (3), CD000980. https://doi.org/10.1002/14651858.CD000980.pub3
- Bae, M., & Kim, H. (2020). Mini-Review on the Roles of Vitamin C, Vitamin D, and Selenium in the Immune System against COVID-19. Molecules (Basel, Switzerland), 25(22), 5346. https://doi.org/10.3390/molecules25225346
- Abobaker, A., Alzwi, A. & Alraied, A.H.A. Overview of the possible role of vitamin C in management of COVID-19. Pharmacol. Rep 72, 1517–1528 (2020). https://doi.org/10.1007/s43440-020-00176-1
- Hemilä, H., & Chalker, E. (2020). Vitamin C as a Possible Therapy for COVID-19. Infection & chemotherapy. VITC – Clinical: Ascorbic Acid (Vitamin C), Plasma. (2021). Retrieved 30 August 2021, from https://www.mayocliniclabs.com/test-catalog/Clinical+and+Interpretive/42362