
Journal of Vita Columbia Volume 2 Issue 1 – Clinical Nutrition
Vitamin D: Overview, metabolism, deficiency and supplementation
January 17th, 2022
Authors:
Orinami Saiki, Mbbs, Fwacs
VP Grewal, MD
How to cite this article:
Saiki O and Grewal VP. Vitamin D: Overview, metabolism, deficiency and supplementation. 2022. Journal of Vita Columbia. 2(1).
Abstract:
Vitamin D is a hormone primarily responsible for bone and calcium metabolism. It also has other extra-skeletal effects; vitamin D receptors are present in almost all parts of the body.1 Vitamin D is primarily obtained from sunlight through the action of Ultraviolet B(UVB) radiation; it is also gotten from plant sources. Vitamin D in whatever form is converted to its active form 1,25 cholecalciferol in the kidney. Vitamin D deficiency has serious implications on the body; it affects the musculoskeletal system, immunity and cardiovascular system. Its deficiency has also been linked to the development of some cancers.1 Due to the role played by Vitamin D in these Organs and systems, it is essential that its deficiency is treated, and when required, individuals should have vitamin D supplementation.
Introduction:
Vitamin D is a steroid hormone responsible for bone and calcium homeostasis. However, some other studies have identified its role in other extra-skeletal activities like cardiovascular disease and autoimmune diseases.1,2 There have even been more recent concerns regarding the role of vitamin D deficiency in causing chronic lung fibrosis; this has significant relevance in patients with COVID 19 disease.3,4
Metabolism of Vitamin D:
Vitamin D is a fat-soluble hormone and exists in two forms. The first form is vitamin D3 which animals produce from the skin, and Vitamin D2 produced by plants.5 Vitamin D is produced in the skin from 7-dehydrocholesterol(7DHC), an intermediate of cholesterol through the action of Ultraviolet B (UVB) radiation. The synthesis of Vitamin D depends on the concentration of 7-dehydrocholesterol reductase; this enzyme catalyzes the reversible reduction of 7DHC into cholesterol. Vitamin D then undergoes two processes of hydroxylation to be converted to its active form, first in the liver (25 hydroxy Vitamin D) and subsequently in the kidney and other organs by 1-α hydroxylase to 1,25- Dihydroxy Vitamin D, Calcitriol. The action of Vitamin D is by its active form, calcitriol, which acts on vitamin D receptors on cells.5
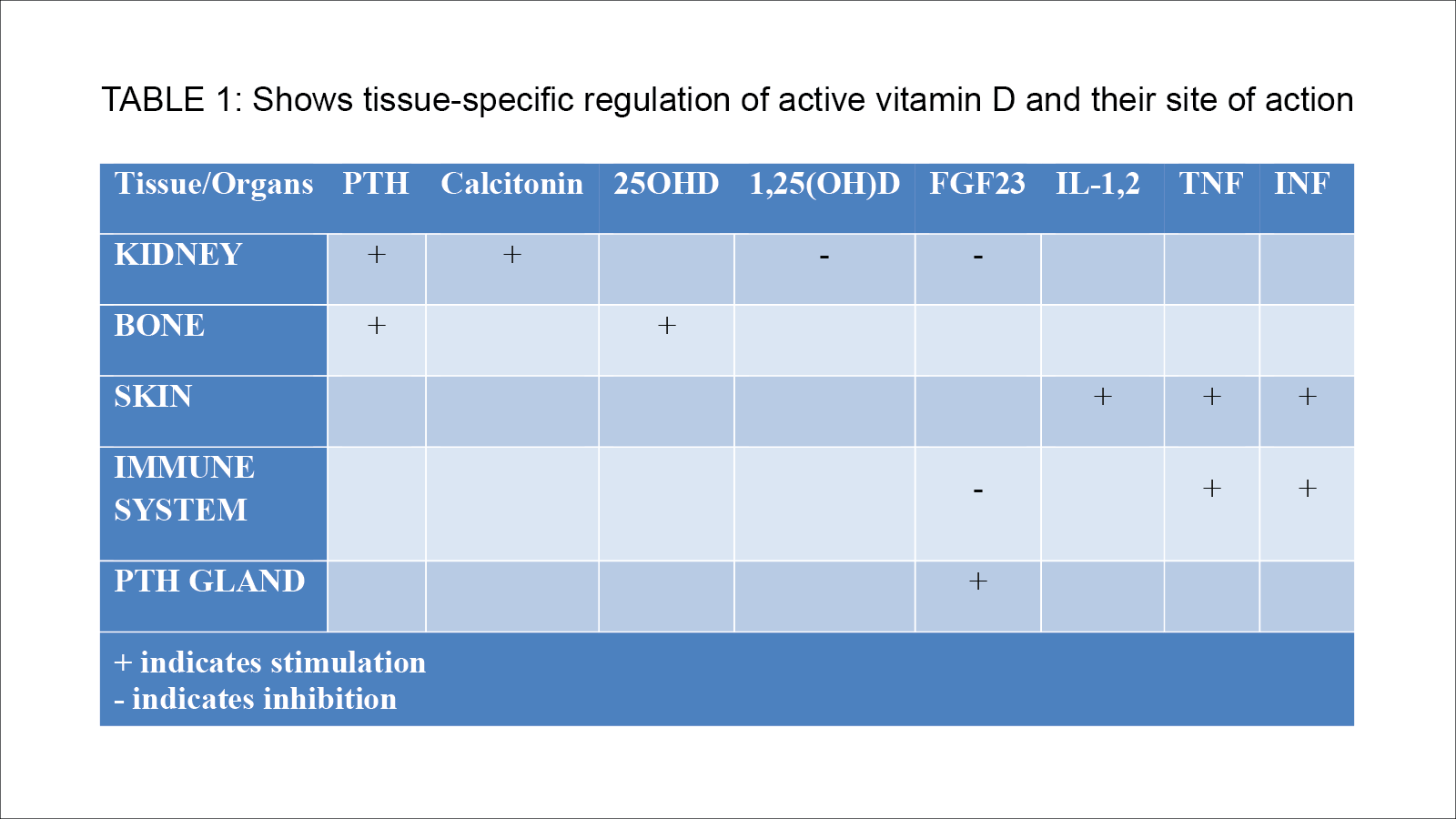
Local production of the active form of Vitamin D have been described in some extra-renal organs such as; Epithelial cells, placenta, bone, brain, liver, endothelial cells and endocrine glands (parathyroid, thyroid, pancreatic islets, adrenal medulla and gonads). Regulation of active vitamin D productions thus occurs within the kidneys and extrarenal.2,5
Vitamin D is classically known for its role in bone and calcium metabolism, including renal calcium absorption, regulation of intestinal calcium absorption and release of calcium and phosphate from the bone. However, in recent times, more researches have been done showing other roles of Vitamin D in multiple organs/system which include; Cardiovascular system, immune system, adipose tissues, glucose/lipids metabolism, muscles and in cancer prevention.2,5
Cardiovascular system: Vitamin D has been shown to have a direct effect on cardiomyocytes and vasculature. Low vitamin D level has been associated with an increased risk of cardiovascular diseases such as hypertension, stroke, heart failure, coronary artery disease and ischaemic artery disease. A low level of Vitamin D has also been found to affect the prognosis of patients with cardiovascular diseases adversely.6,7
Immune System: Vitamin D plays a major role in the immune system ( innate and acquired). It stimulates production of IL-10, which has anti-inflammatory properties. It also decreases the release of pro-inflammatory cytokines such as IL-6 and TNFα. Vitamin D deficiency has been associated with increased risk of infection and autoimmune diseases.8,9 A large meta-analysis has shown that vitamin D prophylaxis prevented the development of acute respiratory infections in adults. These findings establish a pedestal for further research on the role of Vitamin D in the prevention of SARS-COV2 infections.10 Some studies have reported low vitamin D levels in patients being treated for COVID-19 infection, and those with these low levels had worse prognosis. The role of vitamin D in preventing acute respiratory infection may be due to its immune function and also the fact that respiratory infection occurs more during the winter when there is no sunshine, thus affecting vitamin D production.3,4
Glucose/Lipid metabolism: low level of vitamin D has been associated with metabolic syndrome. Vitamin D receptor has been found to be present in all cells responsible for both type 1 and 2 diabetes mellitus. A low level of Vitamin D level has been reported as a risk factor for development of diabetes mellitus in animal models, though this is yet to be substantiated in human studies.11
Muscle: It has also been reported that vitamin helps to improve muscle strength and function in both adults and children.12,13
Cancer: Vitamin D receptors have been expressed in some cancer cell lines, and it has been studied for its role in cancer. Vitamin D has been proven to have an anti-proliferative effect on melanoma, myeloma cells, and other cancer cell lines. However, its role on cancer is still controversial as more studies is being carried out.14,15
Vitamin D Deficiency:
Vitamin D deficiency is a global problem affecting over 1 billion children and adults worldwide.2 Its deficiency is associated with adverse acute and chronic medical conditions, which include: Dental caries in childhood, preeclampsia, cardiovascular diseases, autoimmune disorders, infectious diseases, type 2 Diabetes mellitus, some malignancies and neurological diseases.1,2 Vitamin D deficiency may also cause muscle weakness, bone loss, rickets in children, and increased fracture risk.
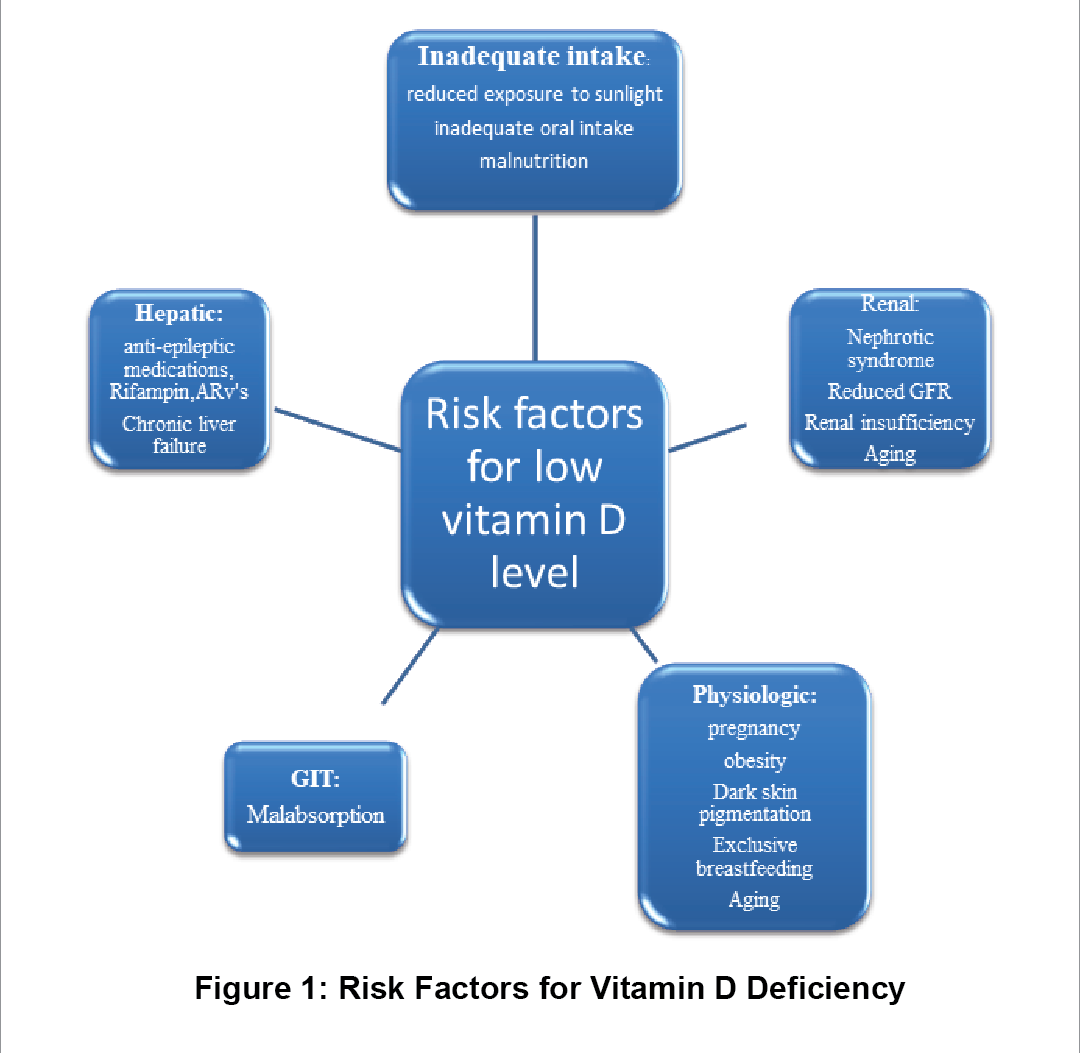
There are some risk factors for Vitamin D deficiency, the diagram below illustrates the various risk factors for vitamin D deficiency. Vitamin level is measured using 25(OH) D levels, a level of less than 20ng/ml is considered low.
Treatment of Vitamin D Deficiency:
Vitamin D is primarily gotten from sunlight; however, some can be gotten from plant sources. Both D2(Ergocalciferol) and D3(Cholecalciferol) are available as dietary supplements.1,2,16 Vitamin D2 is found in some mushrooms while vitamin D3 is found in oily fish, fish liver oil and egg yolk. Vitamin D supplementation is necessary to improve musculoskeletal health and also to decrease mortality from cardiovascular diseases and cancers.16
The national institute of health recommends a daily intake of 400-800IU/day to maintain optimum vitamin D17 level though some other studies recommend as much as 1000-4000iu/day to maintain optimum level.16 However, the amount of vitamin D supplement needed will also depend on other factors such as age, ethnicity, clothing, sun exposure, season and latitude.
Several clinical studies on Vitamin D in pregnancy have reported high prevalence of Vitamin D deficiency in pregnancy with associated adverse effects on the mother and baby.18,19 On the other hand, a couple of randomized controlled trials have showed inconsistent findings.20 Notwithstanding, currently a daily dose of 400-800iu/day of vitamin D is recommended for pregnant women, although some other studies recommend as high as 800-1200iu/day.18
Vitamin D supplementation is also required in the paediatric population in doses ranging from 1000-4000iu/day. Vitamin D supplementation is particularly needed in children with the following conditions; Obesity, cystic fibrosis, insulin resistance, type 1 DM and celiac disease.21
There are still contrasting findings from studies on the role of routine Vitamin supplementation in the prevention of acute respiratory infection. The beneficial effect of vitamin D supplementation in this regard is yet to be proven.22,23
Vitamin D supplementation has also been recommended in some studies for postmenopausal women, reducing falls and improving muscle function.16
It is important that barring all circumstances, Vitamin D level should be maintained to at least 20ng/ml which is the minimum required level, although some researchers report that a level of 30ng/ml and above is the adequate optimal level.1,2
Vitamin D Toxicity:
Vitamin D toxicity is a very rare phenomenon. Excessive exposure to sunlight is not responsible for toxicity. 1,2 Toxicity is caused by either intentional or non-intentional intake of vitamin D supplements for long periods, this leads to excessive absorption of calcium. Its very important for people to know the various doses and accurate unit of measurement of vitamin D supplements. This could present as nausea, vomiting. dehydration, kidney stones, muscle weakness and confusion. Extreme cases of toxicity can lead to renal failure, arrhythmias and death.
Conclusion:
Vitamin D is a very important hormone for maintaining musculoskeletal health and other vital functions in the body. The deficiency of Vitamin D is prevalent worldwide and can cause serious effects on the musculoskeletal system, cardiovascular system, immunity and other body functions. It is essential that vitamin supplements be taken to maintain normal levels in the body to help preserve its functions.
References:
- Kennel KA, Drake MT, Hurley DL. Vitamin D deficiency in adults: when to test and how to treat. Mayo Clinic Proceedings. 2010 Aug;85(8):752-7; quiz 757-8. DOI: 10.4065/mcp.2010.0138. PMID: 20675513; PMCID: PMC2912737.
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord 18, 153–165 (2017). https://doi.org/10.1007/s11154-017-9424-1.
- Carpagnano, GE., Di Lecce V, Quaranta, VN. et al.Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J Endocrinol Invest 2021;(44): 765–771. https://doi.org/10.1007/s40618-020-01370-x
- Radujkovic A, Hippchen T, Tiwari-Heckler S, Dreher S, Boxberger M, Merle U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients [Internet] 2020;(12):2757. Available from: http://dx.doi.org/10.3390/nu12092757
- Saponaro F, Saba A, Zucchi R. An Update on Vitamin D Metabolism. International Journal of Molecular Sciences [Internet] 2020;(21):6573. Available from: http://dx.doi.org/10.3390/ijms21186573
- Wang L, Song Y, Manson JE, Pilz S, März W, Michaëlsson, K, Lundqvist A, Jassal SK, Barrett-Connor E, Zhang C et al. Circulating Levels of 25Hydroxy-Vitamin D and Risk of Cardiovascular Disease: A Meta-Analysis of Prospective Studies. Circ. Cardiovasc. Qual. Outcomes 2012; (5): 819–829.[CrossRef]
- Judd SE, Tangpricha, V. Vitamin D deficiency and risk for cardiovascular disease. Am. J. Med. Sci. 2009;(338): 40–44. [CrossRef]
- Martens P J, Gysemans C, Verstuyf A, Mathieu C. Vitamin D’s Effect on Immune Function. Nutrients 2020;(12): 1248. [CrossRef] [PubMed]
- Colotta F, Jansson B, Bonelli F. Modulation of inflammatory and immune responses by vitamin D.J. Autoimmun. 2017;( 85): 78–97. [CrossRef] [PubMed]
- Martineau AR, Jolli_e DA, Hooper RL, Greenberg L, Aloia JF, Bergman P, Dubnov-Raz G, Esposito S, Ganmaa D, Ginde A.A, et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017; 356: i6583.[CrossRef]
- Mathieu C. Vitamin D and diabetes: Where do we stand? Diabetes Res. Clin. Pract. 2015; (108): 201–209.[CrossRef] [PubMed
- Bischo_-Ferrari HA,Dawson-Hughes B, Baron JA, Burckhardt P, Li R, Spiegelman D, Specker B, Orav JE, Wong JB, Staehelin HB,et al. Calcium intake and hip fracture risk in men and women:A meta-analysis of prospective cohort studies and randomized controlled trials. Am. J. Clin. Nutr. 2007;(86):1780–1790. [CrossRef]
- Bischo_-Ferrari HA. Relevance of vitamin D in muscle health. Rev. Endocr. Metab. Disord. 2012;(13): 71–77.[CrossRef]
- Colston K, Colston MJ, Feldman D. 1,25-dihydroxyvitamin D3 and malignant melanoma: The presence of receptors and inhibition of cell growth in culture. Endocrinology 1981;(108): 1083–1086. [CrossRef]
- Duffy MJ, Murray A, Synnott NC, O’Donovan N, Crown J. Vitamin D analogues: Potential use in cancer treatment. Crit. Rev. Oncol. Hematol. 2017;(112): 190–197. [CrossRef]
- ZhangY, Fang F, Tang J, Jia L, Feng Y, Xu P et al. Association between vitamin D supplementation and mortality: systematic review and meta-analysis BMJ 2019; (366) :l4673 doi:10.1136/BMJ.l4673
- Office of dietary supplements-Vitamin D (2021, July 28). National Institute of health. https://ods.od.nih.gov/factsheets/VitaminD-Consumer/
- Pilz S, Zittermann A, Obeid R, Hahn A, Pludowski P, Trummer C, et al. The Role of Vitamin D in Fertility and during Pregnancy and Lactation: A Review of Clinical Data. International Journal of Environmental Research and Public Health [Internet] 2018;15:2241. Available from: http://dx.doi.org/10.3390/ijerph15102241
- Hollis BW, Wagner CL. New insights into the vitamin D requirements during pregnancy. Bone Res. 2017;(5): 17030. [CrossRef] [PubMed]
- Cooper C, Harvey NC, Bishop NJ, et al. Maternal gestational vitamin D supplementation and offspring bone health (MAVIDOS): a multicentre, double-blind, randomized placebo-controlled trial. Lancet Diabetes Endocrinol2016; (4):393–402.
- Cediel G, Pacheco-Acosta J, CastiUo-Durdn C. Vitamin D deficiency in pediatric clinical practice. Archivos Argentinos de Pediatria. 2018 Feb;116(1): e75-e81. DOI: 10.5546/aap.2018.eng.e75. PMID: 29333826.
- Martineau AR, Hanifa Y, Witt KD, et al. Double-blind randomized controlled trial of vitamin d3 supplementation for the prevention of acute respiratory infection in older adults and their carers (ViDiFlu). Thorax 2015; (70):953–960.
- Denlinger LC, King TS, Cardet JC, et al. Vitamin d supplementation and the risk of colds in patients with asthma. Am J Respir Crit Care Med 2016;(193):634–641.